Abstract
Case Study
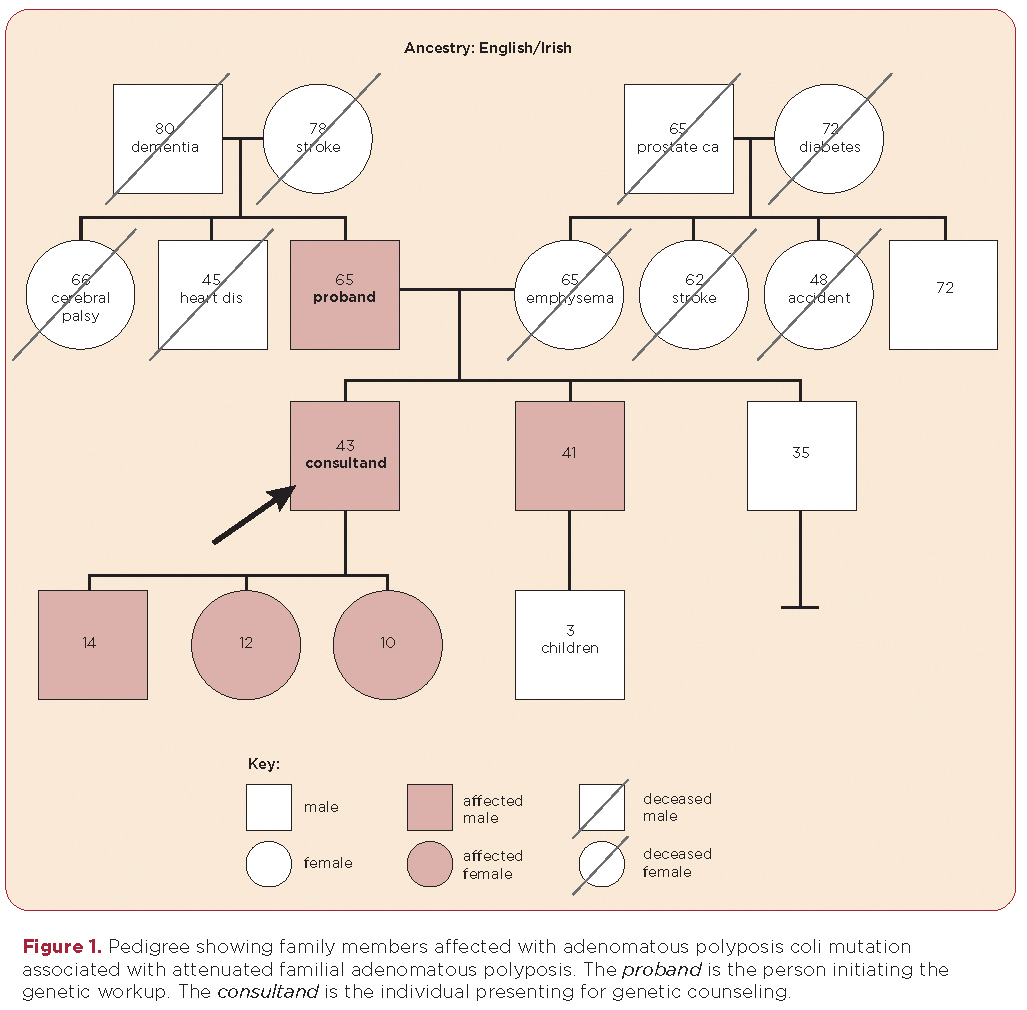
D.R. is a healthy 42-year-old male who presented to the High Risk Familial Cancer Clinic because his father had been recently diagnosed with attenuated familial adenomatous polyposis. His father, L. R., age 65 years with a history of hypertension and heart failure, had visited his primary care practitioner (PCP) complaining of fatigue. His PCP obtained a complete blood cell count and examined his stool for occult blood. L.R. was found to have microcytic anemia (hemoglobin of 8.6/dL, hematocrit of 25.8%, mean corpuscular volume of 76 fL) and guaiac-positive stools; his PCP referred him for a colonoscopy. Although L.R. was 65 years old, this was his first colonoscopy. Over 100 polyps with variable pathology were identified throughout the colon and rectum, including hyperplastic polyps and tubular and tubulovillous adenomas. The largest tubulovillous adenoma was 1 cm. L.R. was referred for genetic counseling and, after informed consent was obtained, underwent testing for familial adenomatous polyposis. The test results showed a deleterious mutation in the adenomatous polyposis coli gene (exon 4:c.426_427delAT). L.R. underwent a total proctocolectomy with ileal pouch anal anastomosis. After receiving genetic counseling, D.R. received site-specific testing for the genetic mutation identified in his father and subsequently tested positive for the same mutation. Of note, D.R. has three children, ages 10, 12, and 14. All three children tested positive for the same mutation (see pedigree in Figure 1).