Abstract
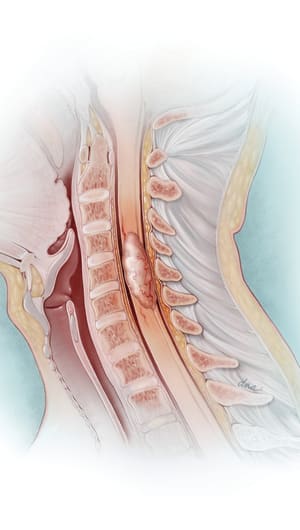
A 24-year-old African American female (L.R.) with a history of smoking and gestational diabetes was diagnosed with Hodgkin lymphoma. She received multiple chemotherapies, including six cycles of ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine), followed by radiation therapy to left inguinal areas for a total of 30.6 Gy in 17 fractions; she obtained complete remission. Two years later, L.R. had disease relapse in the mediastinum and received two cycles of ESHAP (etoposide, methylprednisolone, high-dose cytarabine, cisplatin) followed by etoposide and ifosfamide. She then received BEAM (carmustine, etoposide, cytarabine, and melphalan) as a conditioning regimen and underwent autologous bone marrow transplant. Her post-transplant course was complicated by cytomegalovirus antigenemia, aspergillus pneumonia, and congestive heart failure with left ventricular ejection fraction (LVEF) of 20%–25%. She was treated with an ACE inhibitor (lisinopril) and a beta-blocker (carvedilol) with improvement of her LVEF to 30%–35%. A follow-up chest x-ray showed an increase in the size of the anterior mediastinal adenopathy suspicious for relapse of lymphoma, and at the same time she was also found to be 5 weeks pregnant.
Given her cardiomyopathy, significant obesity, poorly controlled diabetes, and cancer recurrence, L.R. was advised by her gynecologist that the pregnancy was very high risk and might not be viable. The oncologists advised her to terminate the pregnancy within the first trimester, as she needed salvage radiotherapy treatment to the mediastinum and chemotherapy treatments that might endanger the fetus. However, the patient decided to continue with the pregnancy. A multidisciplinary team—which included a cardiologist, oncologist, high-risk obstetrician, pharmacist, and nurse practitioner—was then involved to provide care during the pregnancy. A social worker was also solicited to help with home and financial issues because L.R. was a single mother with a 2-year-old son.
L.R. was treated with carvedilol and furosemide, with monthly cardiology clinical follow-up during the first and second trimesters, then every 2 weeks starting with the 28th week, and weekly thereafter until delivery. Between visits, she notified the clinic for symptoms of heart failure exacerbation and was seen as necessary. The possible in utero effects of both medications were discussed with the patient. L.R. had a normal uncomplicated pregnancy and delivered a 6-pound, 10-ounce healthy boy at 39 weeks via vaginal delivery and was discharged home 2 days later.
A week after delivery, L.R. presented to the cardiology clinic in good spirits and was excited to show pictures of her newborn baby. She had no cardiac complaints and the repeat echocardiogram showed an unchanged LVEF of 30%–35%.