Abstract
Case Study
In February 2011, a 69-year-old, 1.91 m2 Caucasian male was diagnosed with acute myeloid leukemia (AML). Immediately prior to the diagnosis of AML, the patient was otherwise healthy until he developed multiple infections, including what was reported as combination viral and bacterial upper respiratory infections. The patient also developed a dental abscess after food became lodged between a molar and gum, which was unable to be drained; therefore, the patient was placed on antibiotics, and an internist ordered a complete blood cell count (CBC). The CBC revealed leukocytosis with 24,500 white blood cells (WBC)/mm3, hemoglobin (Hgb) 10.8 g/dL, and a platelet count of 17,000/mm3. The patient said he experienced excessive bleeding from his gums and expressed exudative material from the abscess.
When diagnosed, the patient had 50% to 60% monoblasts/promonocyte with 30% monoblasts in peripheral blood. The monoblasts were positive for CD33, dim CD13, dim CD64, dim CD14, CD11c, and CD11b. On immunophenotypic analysis, the percentage of abnormal cells was 60% to 65%. CD34, CD117, and human leukocyte antigen (HLA)-DR were not expressed. The T cells showed no pan T-cell antigenic deletion or diminution and no CD4/CD8 subset restriction. FMS-like tyrosine kinase 3 (FLT3) and nucleophosmin (NPM1) were not mutated.
The patient underwent induction chemotherapy after the initial diagnosis consisting of “7+3” with cytosine arabinoside at 100 mg/m2 continuous intravenous infusion for 7 days and idarubicin at 12 mg/m2 intravenously (IV) on days 1 through 3. The patient’s induction regimen at that time was and is currently widely accepted as the current standard of care. The patient tolerated the induction therapy well and had no evidence of tumor-lysis syndrome. A bone marrow aspiration was performed on day 14, which is the standard of care for monitoring after induction therapy. The bone marrow aspiration showed virtual aplasia, and flow cytometry did not show blasts. The patient received transfusion support as needed. The patient then underwent four cycles of high-dose cytosine arabinoside consolidation and tolerated the treatment well. After induction and consolidation therapies, the bone marrow extraction was negative for residual or recurrent leukemia.
Patient Presents With Symptoms
In October 2014, approximately 3 years following initial diagnosis and remission, the patient presented to his oncologist with a low-grade fever and a 2.3-kg weight loss within the past week attributed to decreased oral intake, oral pain, and edema, which resulted in a weight of 99.3 kg. The patient saw his primary care physician the previous day, and a CBC was obtained; it revealed remarkable leukocytosis with 121,000 WBC/mm3, hemoglobin of 4.8 mg/dL, and a platelet count of 15,000/mm3. Six weeks prior to presentation, the patient had traveled to Missouri and developed fatigue and intermittent chest pain, particularly on exertion, with exertional dyspnea and palpitations 3 weeks later. The patient was admitted to the hospital for transfusion, bone marrow aspiration with core biopsy, and to repeat induction chemotherapy.
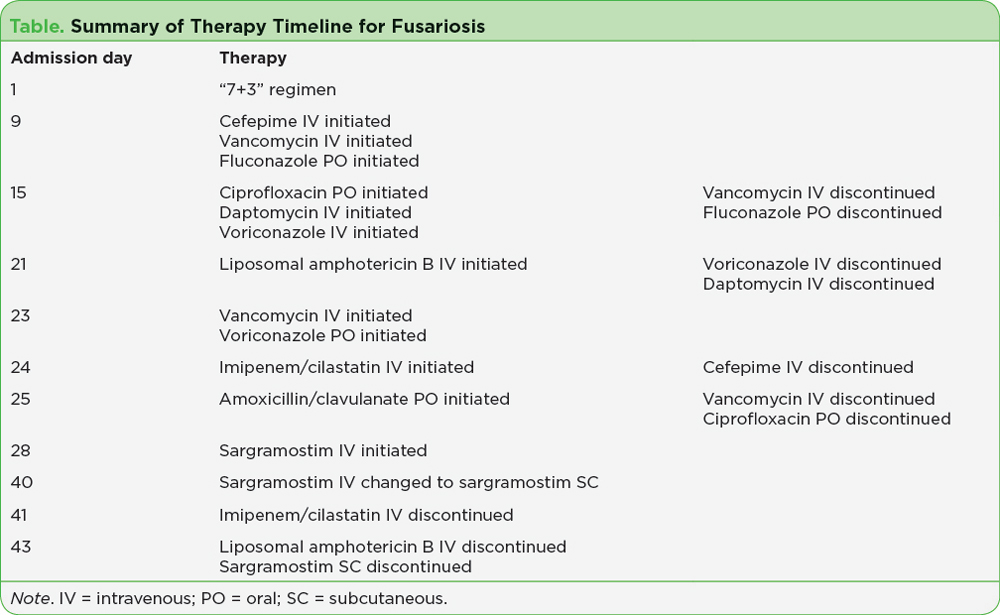
On day 9 of admission, the patient developed neutropenic fever without an obvious source. The CBC revealed 400 WBC/mm3 with an absolute neutrophil count (ANC) of 88/mm3 and a maximum temperature of 38.7°C. The patient believed he suffered a spider wound while he was visiting in Missouri. The area was initially red, with a small fluid-filled blister and was healing on his right arm but remained tender. An infectious diseases physician was consulted, and the patient was subsequently initiated on broad-spectrum antimicrobial therapy consisting of intravenous cefepime and vancomycin, as well as oral (PO) fluconazole at 200 mg daily. Blood cultures, urine cultures, procalcitonin, histoplasmosis antigen, and Aspergillus Galactomannan antigen were collected. All serology testing performed was negative.
On day 15 of admission, the right arm cellulitis was largely unchanged, with continued intermittent fevers. Cefepime therapy was continued, but other pharmacologic therapy was adjusted to add high-dose oral ciprofloxacin, intravenous vancomycin was changed to intravenous daptomycin, and oral fluconazole was changed to intravenous voriconazole at 6 mg/kg every 12 hours. All cultures and antigen tests continued to yield negative results; however, fever in the setting of profound neutropenia continued. Due to a concern for an atypical infection, a punch biopsy for diagnosis was obtained on day 16 of admission, and the patient underwent irrigation and debridement of the right arm.
Confirmation of Fusarium Infection
Cultures collected from irrigation and debridement of the arm confirmed Fusarium species infection on day 21 of admission. The patient underwent wide-margin surgical resection of the locally invasive lesion, and there was no evidence of any hematogeneous spread. Due to concern for resistance to azole therapy, intravenous liposomal amphotericin B was initiated at 5 mg/kg every 24 hours on day 21 of admission, and voriconazole was then discontinued, along with daptomycin.
A right cellulitis leg wound appeared and was noted on day 23 of admission. The area was not improving, which raised concern for dissemination of Fusarium infection. Empiric gram-positive organism coverage with intravenous vancomycin was also added due to the worsening right leg cellulitis. Oral voriconazole was also resumed in addition to liposomal amphotericin B at a dosage of 300 mg every 12 hours for 2 days. The dosage of voriconazole was decreased to 200 mg every 12 hours for 5 days and subsequently increased back to 300 mg every 12 hours for the duration of the admission. Liposomal amphotericin B therapy was continued for 21 days total in combination with voriconazole.
On day 24 of admission, the patient developed a nonproductive cough and bilateral pulmonary infiltrates with spiculated masses seen on a noncontrast chest computed tomography (CT). This raised concerns for atypical fungal pneumonia. Due to the physician’s concern for Nocardia species, cefepime therapy was changed to intravenous imipenem/cilastatin, which was continued for 14 days. The patient had persistent neutropenia and developed worsening renal function. After 2 days of broadening antimicrobial therapy, the cough improved slightly.
The patient’s cough and chest x-ray displayed improvement on day 27 of admission and therefore revealed an alternate source of infection than Fusarium species. After 3 days of vancomycin therapy, there was no Staphylococcus aureus isolated, and vancomycin therapy was changed to amoxicillin/clavulanic acid. The patient also received recombinant granulocyte macrophage colony-stimulating factor support with sargramostim at 500 mg, equivalent to approximately 218 mg/m2/day, IV infusion every 24 hours for 2 weeks, as the product is labeled for AML following induction chemotherapy. The route was subsequently changed to sargramostim subcutaneous (SC) at 500 mg every 24 hours for 4 days.
The patient’s condition began improving significantly with his absolute neutrophil count ≥ 1,000 (1,164/mm3) on admission day 40. He was then transferred to the physical rehabilitation unit due to significant deconditioning during the 49-day inpatient admission. The patient received physical rehabilitation for 7 days and was then discharged home on amoxicillin/clavulanic acid for 7 additional days for the leg cellulitis and treatment with oral voriconazole at 300 mg every 12 hours for at least 1 year. The duration of voriconazole following fusariosis is not clearly defined in the published literature, but it was determined the patient should continue the agent for an extended period secondary to the severity of the infection and severe immunosuppression. The patient continued to follow up with the oncology, surgical, and infectious diseases specialists after discharge (see Table at right).